 The chief problem encountered with the treatment of hands and feet by Botox injections is the intense pain associated with the needle puncture into the densely innervated skin of these regions. The traditional technique performed to alleviate pain during Botox injection with needle is the nerve block of the wrist. The potential complications of a nerve block are nerve or vessel damage and temporary loss of hand dexterity. For this reason, many physicians who contentedly treat axillary hyperhidrosis, hesitate to treat palmar hyperhidrosis with Botox. The chief problem encountered with the treatment of hands and feet by Botox injections is the intense pain associated with the needle puncture into the densely innervated skin of these regions. The traditional technique performed to alleviate pain during Botox injection with needle is the nerve block of the wrist. The potential complications of a nerve block are nerve or vessel damage and temporary loss of hand dexterity. For this reason, many physicians who contentedly treat axillary hyperhidrosis, hesitate to treat palmar hyperhidrosis with Botox.
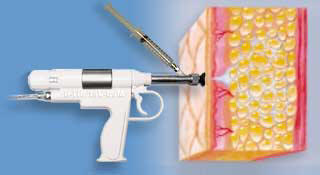
The technique of jet
anesthesia is the
injection of a tiny
amount of lidocaine
<0,1 ml through a
pressurized jet
injector. There are
many benefits to
this
technique :
·
The volume of
lidocaine used is
very small
·
Analgesia is
immediate
·
Jet-injection is
dispersed more
extensively into the
dermis than a needle
injection. Needle
injection tends to
pool along the
needle track alone.
It is assumed that
the spatial
three-dimensional
reconstruction of
the jet injected
liquid has a bulb
shaped distribution
with the broad side
facing the muscle
fascia and the
narrow side
underneath the
epidermis . The
broader spread of
jet injection also
paves the way for a
better diffusion of
the needle injected
Botox that follows,
helping it to reach
a greater number of
eccrine glands,
hence better control
of hyperhidrosis.
·
Jet injection
increases tissue
pressure into the
dermis and
compresses blood
vessels resulting in
reduced bleeding,
contrary to the
nerve block
technique where the
reactive hyperemia
increases the
tendency to bleed
from the injection
sites and causes
some waste of Botox
through reflux.
·
The average pain
score reported by
most patients is
about 2 on a scale
of 0 to 10 where 0
indicates no pain
and 10 indicates the
worst possible pain.
Some patients
reported that the
pain during jet
injection is less
than the needle
injection of Botox
for axillary
hyperhidrosis.
·
Vagal symptoms occur
less frequently with
this technique than
the nerve block
technique and, when
they do, they are
much milder.
Jet injection of Botox directly with Med-Jet into the skin in the treatment of palmar hyperhidrosis |



